ECOSHELTA has long been part of the sustainable building revolution and makes high quality architect designed, environmentally minimal impact, prefabricated, modular buildings, using latest technologies. Our state of the art building system has been used for cabins, houses, studios, eco-tourism accommodation and villages. We make beautiful spaces, the applications are endless, the potential exciting.
By R. Abe. Wingate University.
You quality 100 mcg synthroid medicine 0829085, as read- ers and leaders synthroid 50 mcg line medications made from animals, should use this text as a resource and framework for under- Healthcare Quality and the Patient 23 standing the connectivity of multiple aspects of healthcare quality from the science base, patient perspective, organizational implications, and envi- ronmental effects. This chapter, specifically, sets the stage by highlighting • The current state of healthcare quality; • The importance of the patient in goals and results; • Promising evidence of the great capacity for significant improve- ment in systems of care; • Examples of breakthrough improvements happening today; and • The call to action for all healthcare stakeholders to continue to rethink and redesign our systems for better health for all. Building on this chapter, the book will outline healthcare quality similar to the levels of the healthcare system outlined by IOM. Identify five ways in which you can put the patient more in control of his or her care. Think of an experience you have had with healthcare or one of your family or friends. You are the CEO of your hospital and the local newspaper has just run a story on how bad healthcare is. This patient story was edited by Matthew Fitzgerald, chief scientist, Delmarva Foundation, and originally composed by Heidi Louise Behforouz, M. The Definition of Quality and Approaches to Its Assessment, Volume I: Explorations in Quality Assessment and Monitoring. CHAPTER 2 BASIC CONCEPTS OF HEALTHCARE QUALITY* Leon Wyszewianski Not everyone perceives quality of healthcare services in quite the same way. These physicians had been in the community for at least 25 years each and were known for their dedication and devotion. Their willingness to travel to remote loca- tions without regard to time of day or weather was legendary, as was their generosity toward patients who had fallen on hard times and were unable to pay their medical bills. The emergency department rated number one by the panel was known mostly for its crowded conditions, long waits, and harried and often brusque- mannered staff. Several concepts can help make sense of these and similar apparent contra- dictions and inconsistencies in perceptions of quality of care. This chapter focuses on such concepts, first in relation to the definition of quality of care, and second in relation to its measurement. As we will see, different groups involved in healthcare— in particular physicians, patients, and health insurers—tend to attach different levels of importance to particular attributes and as a result define quality of care differently (see Table 2. The Definitional Attributes The following attributes relevant to the definition of quality of care will be discussed below: • Technical performance; • Management of the interpersonal relationship; • Amenities of care; • Responsiveness to patient preferences; • Efficiency; and • Cost effectiveness. Technical Performance Quality of technical performance refers to how well current scientific med- ical knowledge and technology are applied in a given situation. It is usu- ally assessed in terms of the timeliness and accuracy of the diagnosis, appropriateness of therapy, and skill with which procedures and other med- ical interventions are performed (Donabedian 1980, 1988a). Management of the Interpersonal Relationship The quality of the interpersonal relationship is determined by how well the clinician relates to the patient on a human level. The quality of the interpersonal relationship is also important because of how it can affect technical performance (Donabedian 1988a). A clini- cian who relates well to a patient is better able to elicit from that patient a more complete and accurate medical history (especially with respect to potentially sensitive topics such as use of illicit drugs); that, in turn, can result in a better diagnosis. Similarly, a good relationship with the patient is often crucial in motivating the patient to follow the prescribed regimen of care, such as taking medications or making lifestyle changes, for which noncompliance rates are alarmingly high despite their obvious importance to achieving the ultimate goals of healthcare (Haynes et al. Much like the interpersonal relationship, amenities are valued both in their own right and for their potential effect on the technical and interpersonal aspects of care. Amenities such as ample and convenient parking, good directional signs, comfortable waiting rooms, and tasty hospital food are all of direct value to patients. For exam- ple, in a setting that is comfortable and affords privacy and as a result puts the patient at ease, a good interpersonal relationship with the clinician is more easily established, leading to a potentially more complete patient his- tory and therefore a faster and more accurate diagnosis. Responsiveness to Patient Preferences Although taking into account the wishes and preferences of patients has long been recognized as important to achieving high quality of care, until recently this has not been singled out as a factor in its own right. Basic Concepts of Healthcare Quality 29 Efficiency Efficiency refers to how well resources are used in achieving a given result. Efficiency improves whenever the resources used to produce a given out- put are reduced.
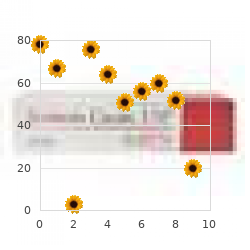
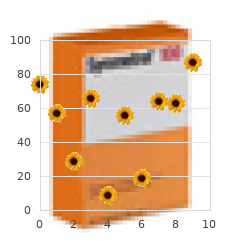
Kaplan–Meier estimates of survival in patients with inoperable hepatocellular carcinoma by double-blind treatment group interval includes the null value of 0 (see also the comparison has an associated two-sided test size comments by Hutton68) order synthroid 50mcg mastercard medicine 2 times a day. For these studies the p-value buy 100mcg synthroid amex medications gabapentin, calculated from the data for the the NNT is not a single number, but varies primary endpoint of the trial, must fall to be according to time since the start of treatment. In this case the null hypothesis of no difference between groups MULTIPLE COMPARISONS is then rejected. In fact for k (assumed independent) outcome measures the false positive tive these issues are reviewed by Proschan and Waclawiw. Clearly, the false positive rate increases as the number of comparisons made increases. SUBGROUP ANALYSIS In order to retain the false positive rate as In designing a RCT, sample size is usually deter- 100α% the Bonferroni correction is often sug- mined by considering a clinically worthwhile gested. This implies only declaring differences as effect which will be estimated from the trial data statistically significant at the 100α% level if the by a comparison of all patients randomised to one observed p-value <α/k. Equiv- that the precision with which this effect size is alently, and preferably, multiply the observed p- estimatedmaybeimprovedbyastratifiedanal- value by k and declare this significant if less ysis adjusted for baseline prognostic variables than α. However, if treat- One approach that has been used to overcome this ments are compared within these strata (thereby difficulty is to quote 99% CIs rather than 95% CIs ignoring information on patients not in that stra- whenever more than a single outcome is regarded tum) it is clear that the patient numbers must be as primary. Thus any such Study Group70 report 21 distinct endpoints, comparisons will usually lack sufficient statistical ranging from fatal myocardial infarction to death power and hence may be unreliable. In some cir- between taking no account of the multiplicity cumstances, one of these subgroup comparisons and retaining 0. For example, Green22 highlights group analysis can appear to favour one treatment this problem with respect to trials of a facto- in one subgroup and the other in the other sub- rial design. This may then lead to a false conclusion 38 TEXTBOOK OF CLINICAL TRIALS that the new treatment works for one group but COMPETING RISKS not for the other. If a subgroup analysis is planned for at the design stage, adjustment for this should In some situations, a patient may fail following be built into the sample size considerations. If relapse is the outcome of interest Although the standard of reporting of randomised in the clinical trial, then usually it is the first event controlled trials has improved in many medi- that is of primary importance to the clinician. There are also many situations in 1A monoclonal therapy was thought to be most which inappropriate and substandard analyses are effective against individually dispersed cells and conducted. Particular examples include statisti- less effective against local satellite tumour nod- cal significance tests of pre-randomisation (base- 78 ules or cell aggregates. Since the 17-1A anti- line) variables, often describing demographic and body should be most effective in preventing or patient eligibility criteria in the different treat- delaying distant metastases after surgery, distant ment groups, despite the allocation to groups metastasis as a first event was thus a key endpoint having been made by randomisation so that any 75 in this trial. In the analysis of competing patterns of failure, the Kaplan–Meier method and the associated OTHER MISUSED APPROACHES logrank test are frequently used to estimate TO ANALYSIS the comparative rates of, for example, local recurrence and distant metastasis in patients Anderson76 catalogues some commonly misused receiving alternative treatments for their cancer in approaches used in the analysis of clinical trials. In one, local recurrence These include in, for example, cancer clinical as the first event is taken as the event of trials with dual endpoints of tumour response interest. In this situation, patients who do not and overall survival, the analysis of survival by have a local recurrence, or who have local tumour response itself. In these cases survival is recurrence as a second or subsequent event, compared between those patients who respond irrespective of whether or not they have distant and those who do not. Anderson states categorically that such metastasis as the first event is taken as the event comparisons are wrong unless an appropriate of interest. Similar considerations apply if comparisons are made between groups established on the basis incidence functions and comparisons between of the amount of (protocol defined) treatment groups via the test developed by Gray. Indeed a whole new industry of Clinical Research There are many statistical packages available for Organisations (CROs) has developed to guarantee the summary and analysis of clinical trials and this process. Further, the Regulatory Agencies additional features are continually being added. Information from randomised controlled trials Over the last decades, there have been many provides key information when the pharmaceu- statistical developments that have impacted on, tical and allied industries apply to register a for example, the endpoints that can be assessed, new drug or device with the relevant regulatory the design, size, analysis and summary. The authorities themselves impose include the Kaplan–Meier method for summaris- certain constraints on the way in which trials ing survival time studies, the logrank test and are conducted – these will include basics with most influential of all the associated Cox pro- respect to a justification of a sample size for portional hazards model which allows between- the trial but will also specify standards. The Cox model can also accommodate time-dependent variables, that is variables that PRINCIPLES OF QUALITY DATA are assessed post-randomisation. These devel- MANAGEMENT opments would have remained theoretical in nature but for parallel developments in statisti- In clinical trials, subjects are usually entered cal software.
We had a clear understanding that she was to see both me and Harry Abram in follow-up generic synthroid 50 mcg on line treatment 001. I had been very direct in telling her that I knew of the heparin injections and warned her of the dan- ger associated with her continuing them generic synthroid 50mcg on-line medicine 4211 v. She continued denying she had given herself these injections, even after discharge. I felt uncomfortable continuing to see her, but I had made a pact with Abram to follow one such patient with him—no matter what. She said she had been letting her student nurses practice injections on her, and obviously one of the students must have broken ster- ile technique. He insisted that he was beginning to make headway, despite the abscess occurrence. Once more, I reluctantly agreed to con- tinue to follow Veronica medically. Within a few weeks after the abscess had been drained, Ve- ronica came into the emergency room, and the physician on call admitted her with a fever of 104 degrees. Te next morning when I saw her, her temperature was 102 degrees with a pulse rate of 76 per minute. Again, she denied it straight out, saying she had no explanation for the sudden drop in fever. She told me her menses had been extremely heavy and that was why she showed blood-loss anemia. When she was finally discharged, I gave her written notice that she must find another medical doctor, and I re- signed from her care. Several more months went by, and then I got a call from a hospital in Atlanta. She told the doctor there that I had been treating her for acute leukemia. I shared my failed experiences with him and wished him more luck than I had had in treating Veronica. At that time in my practice, I was enjoying two of the most gripping fantasies young physicians can have—a sense of omnipo- tence and a belief that I could rescue every single patient in distress. I did not see that the only language such patients have is self-infliction. I never learned to translate their language into one that I could understand and accept. Balint is correct that apostolic functions predetermine the choices a physician has. My own apostolic functions preclude my taking on patients who persist in self-inflicted diseases. To those physicians who can treat the Veronicas of this world, I can only say I wish you well. You are a rare breed, and I hope you will record your experiences for all to read. I knew that I lacked the reflexes and clinical tools this broader clinical model would require. It was time for me to retool and learn to listen and to guide and coach patients. Armed with my experiences with Carl Rogers, Joseph Sapira, and the videotaping sessions in Fairhope, I found new methods of interviewing and intervening. Tese methods include: • Having the primary intention of being maximally helpful with each patient. I can lump all of these into what can be called establishing full at- tention and rapport with the patient. If these steps are blocked or not accepted by the patient, the encounters will become dif- ficult, if not impossible. Such a reaction from the patient should strongly suggest that the patient is enjoying secondary gain from being sick. Te next steps, beyond establishing rapport, are directed at as- sisting the patient to discover or recollect what he or she is doing or not doing to produce the symptoms.
Because of this convergence purchase 100 mcg synthroid amex treatment hemorrhoids, above for specialised cutaneous pathways and in descending excitation of the relevant interneurones Chapter 7 for group II pathways order synthroid 125 mcg with mastercard symptoms 5 weeks into pregnancy. There are two may receive feedback reinforcement by impulses reflex patterns from the FRA: the short-latency evokedfromtheplantarcushionduringcontactwith (early) reflexes found in the acute spinal cat, and the ground (see Fig. There are di- There are multiple reasons to group these afferents synaptic reflex pathways (mediating both excitation together (cf. Lundberg, 1973, 1979, 1982): and inhibition to motoneurones) that operate only (i) They have a common action on motoneurones, with conjoint cutaneous and corticospinal inputs i. Lundberg widereceptivefield,which,formuscleafferents, (1973) speculated that the information from skin includes both flexors and extensors. The increased pre- andthismaybeexplainedbecausethedescend- synaptic inhibition of cutaneous afferents observed ing excitation of FRA interneurones (see below) during the dynamic phase of wrist flexion-extension requires information regarding activity in FRA movements in the awake monkey could function pathways. Following Background from animal experiments 389 intercollicular decerebration, FRA excitation (iii) Muscle contraction secondary to stimulation of flexors and inhibition of extensors is sup- of efferentsactivatestheFRAsystem(seeLundberg, pressed, and following an additional midline 1979). The term FRA is probably temwithamultisensoryinputmaythereforebeused a misnomer that has outlived its usefulness (Lund- to reinforce and prolong the descending command. Parallel descend- FRA reflexes ing excitation of FRA pathways mediating inhibition New perspective on the FRA concept to other motoneurone pools (e. Lundberg (1973, 1979) formulated the hypothesis that, during normal movement, pathways medi- Convergence of nociceptive afferents on ating short-latency FRA reflexes could provide selec- FRA interneurones tive reinforcement of the voluntary command from thebrain. Thehypothesisreliedonexperimentalevi- Convergence would facilitate correction of a move- dence for the following findings. Due to spatial facilitation the required nocicep- ion reflex (see above). The strong mutual inhibition between neurones exciting muscles with opposite function is reminiscent of the half-centre organi- FRA-induced excitation of other pathways sation postulated by Graham Brown (1914)togive Strong excitatory effects from the FRAs have been alternating activation of extensors and flexors dur- described on interneurones belonging to different ing locomotion. Accordingly, when DOPA is given reflex pathways: reciprocal Ia inhibition (Chapter 5, after pretreatment by nialamide, stimulation of p. These findings suggest that facil- activation, dependent on the half-centre organi- itation of impulse transmission in the FRA path- sation of the late FRA pathways (see Lundberg, ways evoked by the active movement might have 1979). There is inhibition of pathways mediating long-latency FRA reflexes by pathways mediating short-latency FRA reflexes Pathways mediating long-latency FRA reflexes After DOPA, prolonging a train of FRA volleys delays With DOPA, short-latency FRA reflexes are the onset of the long-latency response, which then depressed and replaced by long-latency responses appears only after the end of the stimulus train. By several lines of evidence indicate that the short- and causing release of transmitter from a noradrenergic long-latency FRA responses are mediated through pathway, DOPA would inhibit pathway X, thereby different pathways (cf. Lundberg, 1979; Schomburg, releasing transmission through the pathway Y (cf. After DOPA, short-latency reflex (i) Primary afferent depolarisation is exerted actions to motoneurones are blocked, but short- mainly on FRA terminals before DOPA, and on Ia latency pathways still have an inhibitory action on terminals after DOPA. A possible functional outcome IPSPs evoked before DOPA are mediated via a pri- of the inhibition of long-latency FRA pathways by vate inhibitory pathway. It has been suggested (Lundberg, 1979) but peripheral afferents and have different central cir- so far without experimental evidence that there is cuits, similar general principles apply to all cuta- also inhibition from the long-latency to the short- neous reflexes. Conclusions (iii) Cutaneous volleys may be produced by electri- cal or mechanical stimuli. Cutaneous volleys contribute to many spinal (iv) Temporal summation or spatial and tem- reflexes. Stimulation of these fields produces ment which afferents are activated and to dis- withdrawaloftheareafromthepotentiallyinju- tinguish responses produced by stimulation of rious stimulus. However, it must be remem- FRA pathways are evoked mainly from afferents bered that an electrical stimulus sufficiently activated during normal movement, though strong to activate nociceptive afferents will also nociceptive afferents may also contribute. These responses may provide positive feedback designed to prolong and reinforce the voluntary command from the brain. Stimuli (v) The half-centre organisation of pathways medi- ating long-latency FRA responses might be Electrical stimuli responsibleforthealternatingactivationofflex- Electrical stimuli to cutaneous nerves ors and extensors during locomotion. Electricalstimulicanbeappliedtocutaneousnerves, which are generally stimulated where the nerve is Methodology superficial, through bipolar surface electrodes with the cathode proximal. The more commonly stimu- Underlying principles lated nerves are the sural nerve behind or just below the lateral malleolus, the superficial peroneal nerve Although the reflex responses evoked by tactile on the dorsal side of the foot proximal to the exten- and nociceptive stimuli are carried by different sor digitorum brevis, the superficial radial nerve on 392 Cutaneomuscular and withdrawal reflexes the inferior part of the radial edge of the forearm, of 1–3 Hz provide the optimal trade-off between the digital nerves of the fingers and toes using ring reflex attenuation and the need to average more electrodes. Electrical stimulation may also be delivered directly to the skin Mechanical stimuli Direct cutaneous stimulation may be delivered Mechanical stimuli have been used to provide infor- through plate electrodes placed over the skin, at a mation about (i) the responses elicited in forearm site where there is no muscle beneath the skin, to and hand muscles from low-threshold mechano- avoid stimulation of muscle afferents.